Central Fill or No?
“… we’re operating on the assumption that central (fill) is a less-expensive way to fill prescriptions. But we haven’t found the exact right measure of this yet.” Director of Pharmacy Operations
Overview
-
- Hospital patient markets require on-demand delivery and resist delays to departure from the hospital.
- Central fill is an on-demand fill system requiring patients to delay delivery or pre-order prescriptions.
- Removing production delays help reduce order-to-counter delivery time.
- In combination with other changes, the in-store production channel can be modified for both on-demand filling and pre-production.
It is possible the price of central fill systems includes a taking of as much prescription value as possible. The break-even point for the system might even closely correspond to the need for added investment. On the other hand, perhaps the system really is just too expensive to buy and operate effectively and efficiently causing hospital pharmacy directors to ponder the above quote.
If price is no option, there remains the question of whether or not central fill is the right solution for hospital markets. Is it the answer to pharmacist frustration and management confusion over the gap between market potential and realization? Is more production capacity the answer?
Management confusion and pharmacist frustration over the market potential-realization gap need not become the stardust of healthcare consultant dreams. Payroll reduction and closing outpatient pharmacy are desperate solutions to avoid.
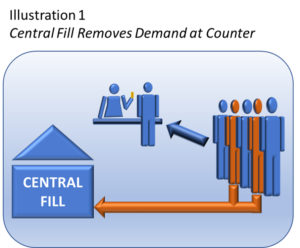
Central fill diverts refill and delayed pick-up away from in-store production demand. This helps reduce in-store labor cost, or under high demand, allows the store to serve more on-demand fills.
Central fill patients must wait for prescription delivery/pick-up and that presents a problem for hospital discharge patients who are often eager to leave for home unless otherwise served by outpatient pharmacy.
The challenge of outpatient pharmacy is immediate delivery capacity not production. Most outpatient pharmacies have plenty of unused production capacity so adding more is not likely to help. The solution requires finding ways to better use this capacity.
Central Fill versus Pre-Production
Vendors consider smaller markets (500+) as potential central fill clients. One could argue whether the scaled down system constitutes true central fill operations or simply a standard production line connected by conveyors and whose only differences are location and manner of delivery.
Although scaled “central fill” still does not address the narrow window of on-demand delivery, the concept of offline production is tantalizingly close to the solution. Effective and efficient delivery models require removal of production time from the fulfillment process. Pre-production of high frequency drugs is part of the answer.
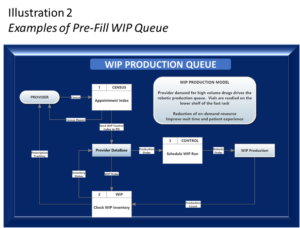
Illustration 2 depicts a provider-based pre-production WIP queue process. Known discharge drug demand drives WIP inventory for high frequency drugs. The pre-packaged inventory complies with FD&C label guidelines[1][2]. WIP accumulates to a pre-determined imminent delivery demand quantity. This inventory is secured in specially designed rack and tray systems.
Combining WIP inventory models with other delivery capacity tools can significantly reduce wait time for patients electing to pick up prescriptions at the outpatient pharmacy counter. The reduced wait time allows more patients into the delivery queue within the narrow window of opportunity.
Combination Production Channel
Customizing the production floor of the pharmacy to allow for both pre-production and high-capacity on-demand fill is likely the least expensive way to solve the on-demand delivery queue issue every outpatient pharmacy faces. Floor layout and fixture design complement other process changes to create a low stress constant rate of production and reduced wait time.

Illustration 3 shows how to integrate the ‘central fill’ conveyor with gravity conveyors to stage current WIP (work-in-process) and move finished product to a packaging station. All WIP is RFD tagged to provided quick access to orders in the channel.
Also serving the production line are WIP racks containing high frequency pre-production medication vials. Special vial trays service the WIP racks to organize inventory and give easy, safe access to the vials.
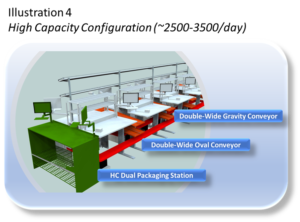
Illustration 4 is similar to Illustration 3 except that it expands the capacity of the production channel with double-wide gravity conveyors, an oval conveyor track, and high capacity packaging station.
Because each station is modular, the production channel easily scales and configures to meet the unique demands of each outpatient pharmacy.
Both configurations are suitable for off-line pre-production runs to replenish the WIP rack inventory. No need for a special facility until economics warrant.
The configurations assume custom, low cost workstations that the hospital’s maintenance/construction staff could easily make and assemble.
Both configurations also include a fast-rack superstructure to support the fill-side workstations. Once again, process changes and variable workflow support the production channel based on changes in demand throughout the day.
Summary
Central fill is a slow way to fill prescriptions and lends itself to markets that do not require immediate or guaranteed delivery. This pretty much rules central fill out for all urgent new prescriptions of the kind hospital markets must serve.
Integrating a robotic, like the new Parata Max 2, with changes in inventory management, process, WIP staging, and conveyance should serve as the starting point for comparison to any central fill options.
Central remains an option for hospital systems to service employees, contracted fills (for other institutions), and patient refills for more robust outpatient in-market operations.
Footnotes
[1] FD&C guidelines all for repackaging and provides guidelines for compliance. It is important that outpatient pharmacies considering pre-production understand the guidance.
[2] While pre-packaging complies with FD&C guideline, drug chains may have blocked hospitals from pre-production through retail bias pharmacy regulations. However, these regulations should be challenged on their merit especially since drug chains have used their considerable leverage to have manufacturers pre-package prescription quantities.